

Abstract
BACKGROUND: Cold agglutinin disease (CAD) is an ultra-rare and potentially life-threatening, acquired autoimmune hemolytic anemia. It is characterized by hemagglutination and hemolysis due to immunoglobulin-mediated (usually IgMᴋ) classic complement pathway activation aggravated by infections and exposure to cold environmental temperatures. As conventional approaches are largely ineffective or short term in controlling hemolysis, complement inhibition (CI) (eculizumab-C5, BIVV009-C1s, and APL-2-C3) represents a novel and promising treatment option in these patients (pts). However, due to inhibition of complement cascade, pts are susceptible to encapsulated bacteria, especially N. meningitidis. Therefore, meningococcal vaccination is mandatory on CI to reduce the risk of infection.
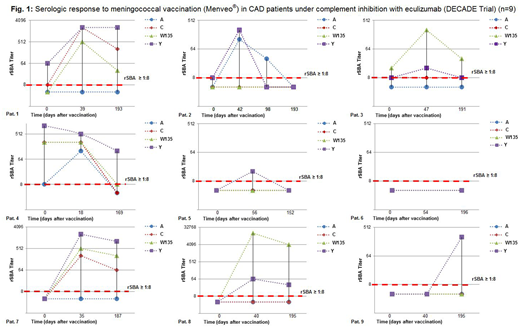
PATIENTS/METHODS: In this systematic study serologic response to the quadrivalent meningococcal polysaccharide conjugate vaccine (Menveo®) in pts with CAD (n=9; 8 females; mean age, 73 yrs (range 64-80 yrs)) was analyzed prior to vaccination and initiation of CI (eculizumab, DECADE Trial (Röth et. al, Blood 2015; 126:274)) and after vaccination at two distinct time intervals (median, 42 days (range 18-60 days) and median, 193 days (range 156-200 days) by measuring serum bactericidal antibody titers with external rabbit complement (rSBA) against meningococcal serogroups A, C, W135 and Y. In one pt rSBA titers were not assessable at the first interval following vaccination. By definition, serologic protection is defined by a rSBA titer ≥1:8 or a fourfold rise pre- to postvaccination.
RESULTS: Serologic response in terms of protective rSBA titers to Menveo® after vaccination varied in CAD pts for the meningococcal serogroups and the different time points: A 25% (2/8), C 25% (2/8), W135 50% (4/8), Y 62% (5/8) at first observation compared to: A 0% (0/9), C 22% (2/9), W135 33% (3/9), Y 44% (4/9) at second rSBA titer measurement, reflecting an early decline in protective rSBA titers to non-protective titers over time (Fig. 1). However, no meningococcal infections have been observed in the analyzed cohort under CI. In pts. with a fourfold rise in rSBA titers pre- to postvaccination the beneficial role of conjugated meningococcal vaccinations in contrast to unconjugated vaccines, resembled by increased immunity with booster vaccinations and an anticipated enhanced duration of protection, might further be supported.
SUMMARY/CONCLUSIONS: Efficiency of meningococcal vaccines for the different serogroups in CAD pts varies significantly and serological response analyses, especially in the currently recruiting CAD-Trials (BIVV009 and APL-2) addressing CI, are useful. By now, revaccination with the tetravalent conjugate vaccine (Menveo®) every 3 years is recommended. However, the associated risks with long-term CI are presently unknown and might be individually based on serologic response analyses to vaccination, which might even imply additional booster vaccination in pts on chronic CI. Physicians and pts must be vigilant for meningococcal infections at all times. A stand-by therapy with ciprofloxacin 750 mg p.o. in case of signs of meningococcal infection should be recommended with immediate medical evaluation and treatment. The availability of the novel vaccines covering serogroup B (Bexsero®, Trumenba®) may further reduce the risk of infections and should be mandatory in these pts, despite no current test exists to measure serologic response to meningococcal serogroup B on chronic CI.
Duehrsen:AbbVie: Consultancy, Honoraria; Amgen: Research Funding; Celgene: Honoraria, Research Funding; Gilead: Consultancy, Honoraria; Roche: Honoraria, Research Funding; Janssen: Honoraria. Röth:Novartis: Consultancy, Honoraria, Research Funding; Amgen: Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Bioverativ: Consultancy, Honoraria; Alexion Pharmaceuticals, Inc.: Consultancy, Honoraria, Research Funding; Roche: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal